Article by Dr Raghuram Y.S. MD (Ay) and Dr Manasa, B.A.M.S
An inguinal hernia is a protrusion of ‘contents of abdominal cavity’ through inguinal canal.
Inguinal canal – There is a canal called inguinal canal which connects the abdomen and the inguinal region (lower part of the belly near the fold between your thigh and scrotum in male and vagina in females). Anatomically inguinal region corresponds to either the ‘groin’ or the ‘lower lateral regions of the abdomen’.
The inguinal canal is a tubular structure that runs infero-medially and contains the spermatic cord in males and the round ligament in the females.
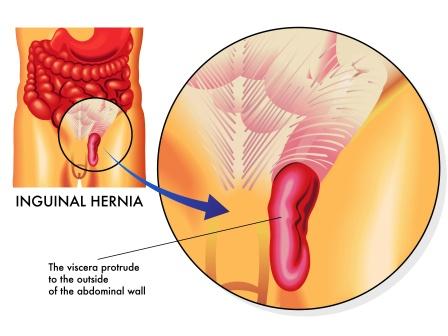
When the abdominal contents, mainly the coils of intestine get displaced and enter the inguinal canal and progress towards the scrotum (bag like structure which holds testicles), they cause a bulge in the groin and scrotum along with pain and discomfort. This condition is called ‘inguinal hernia’.
The symptoms include pain and discomfort, which are mainly evident while coughing, exercise or bowel movements (when pressure moves downwards) and is present in about 66% of affected people.
Symptoms of inguinal hernia worsen throughout the day (often) and improve when lying down. Right sided hernias are more often seen than the left sided ones. When the blood supply to apart of intestine (protruding in the hernia) gets blocked, that part of intestine which is depleted of blood supply gets strangulated. This causes severe pain and tenderness in the afflicted area.
Table of Contents
Causes
Gist of Co-factors or mechanical and chemical causes of ‘Inguinal hernia’

- Any mechanical movement or posture which exerts stress on the abdominal wall or floor
- Acute and or chronic constipation
- Straining bowel movements
- Forcibly pushing down the abdominal gas (flatus, fart)
- Chronic cough
- Violent sneezing
- Excessive eating
- Lifting heavy objects
- Violent exercises and too much athleticism
- Sedentary life, too less exercise
- Incorrect and too frequent bending
- Long distance marathons, cycling and or too much swimming
- Too tight waist belts
- Alcohol and smoking
- Prescription drugs that weaken the digestive system
- Frozen, canned or junk foods, too much nutrient supplements, cold beverages, artificially sweetened sodas
Signs and symptoms
Signs and Symptoms of Inguinal Hernia
Bulge in the groin which
– Becomes prominent when coughing, straining or standing up
– Are rarely painful
– Commonly disappears on lying down
– Gets associated with mild discomfort over a period of time
Incarcerated hernia – When the bulge cannot be reduced or placed back into the abdomen it is said to be ‘incarcerated’. This condition requires emergency surgery.
Strangulated Bowel – It occurs when the blood supply to the part of intestine is blocked. It is a type of incarcerated indirect inguinal hernia. It should be suspected when significant pain is associated with hernia. This may lead to gut ischemia (loss of blood) and gangrene with fatal consequences.
Intestinal obstruction – With the progression of hernia, the abdominal contents such as intestines, liver can descend into the hernia causing an intestinal obstruction.
Risk Factors
- Smoking
- Obesity
- COPD (Chronic Obstructive Pulmonary Diseases)
- Pregnancy
- Collagen vascular diseases
- Peritoneal dialysis
- Previous open appendectomy etc
Hernias are partly genetic. They occur most often in certain families.
It is said that the inguinal hernias are associated with heavy weight lifting but it is not proved.

Diagnosis
Diagnosis is usually done based on signs and symptoms
Medical imaging – used to confirm the diagnosis or rule out the other possible causes
Hernia repair is not needed in groin hernias which do not carry any symptoms. In females repair is generally recommended due to higher rate of femoral hernias which carry lot of complications.
Immediate surgery is needed in case of strangulation.
Open surgery or laparoscopic surgery is the best methods of inguinal hernia repair. Laparoscopic surgery is associated with less pain following surgery.
Types
Types of Inguinal hernia, diagnosis
Inguinal hernias are of 2 types. They are direct and indirect hernias. These types of hernias are defined by their relationship to the inferior epigastric vessels.
Direct inguinal hernia
Direct inguinal hernias occur medial to the inferior epigastric vessels. It enters through a weak point in the fascia of the abdominal wall. To be precise, it protrudes through a weakened area in the transversalis fascia near the medial inguinal fossa within the inguinal or Hesselbach’s triangle. These hernias cannot exit via the superficial inguinal ring. Therefore they cannot extend into the scrotum. It occurs 10 times more in the males than in females. They tend to occur in the middle-aged and elderly people. This is because the abdominal walls weaken with age.
Additional risk factors are –
- Obesity
- Being over-weight
- Chronic cough
- Chronic constipation,
- Family history and
- Prior episodes of direct inguinal hernias
Indirect hernias can occur at any age including the young. This is because they have a congenital component.
Pantaloon Hernia – It is a condition when both direct and indirect hernias are simultaneously present on the same side.
Indirect Inguinal Hernia
This mainly occurs from the failure of embryonic closure of deep inguinal ring after the testicle has passed through it. It protrudes through the superficial inguinal ring.
In male fetus – The peritoneum or the covering of the abdominal viscera provides a coating to the testis as the testis passes through the inguinal ring. This forms a temporary connection called processus vaginalis. The processus vaginalis gets obliterated once the testicle is totally descended. The permanent coat of the peritoneum which later remains around the testicle is called tunica vaginalis. The testicle remains connected to its blood vessels and vas deferens. The blood vessels and vas deferens form the spermatic cord. Along with the spermatic cord the testes descends through the canal into the scrotum.
The deep inguinal ring (beginning part of the inguinal canal) remains as an opening in fascia transversalis. This fascia forms the inner wall of the spermatic cord.
When this opening is larger than necessary (opening should be only large enough to permit spermatic cord and nothing else) the indirect inguinal hernia occurs. The protrusion of peritoneum through the internal inguinal ring can be considered as an incomplete obliteration of the processes.
In the indirect hernia, the protrusion passes through the deep inguinal ring and is located lateral to the inferior epigastric artery.
These are of 3 main types.
Bubenocele – Hernia is limited in the inguinal canal
Funicular – Here processus vaginalis is closed at its lower end (just above the epididymis). The hernia sac contents can be felt separately from the testis. The testis lies below the hernia.
Complete (vaginal) – Here the processus vaginalis is patent throughout. The hernia sac is continuous with tunica vaginalis. The hernia descends down to the bottom of the scrotum. It is difficult to differentiate or palpate the testis and hernia separately.
In women, the hernia eventually reaches the labium majus of the afflicted side. Hernias cause enlargement of one labium if they progress. Indirect hernias are common in women.
Diagnosis is chiefly done on the basis of signs and symptoms, after a thorough examination. Imaging helps in confirmation of the diagnosis. Ultrasound, CT or MRI helps in differentiating indirect hernias from spermatic cord lipomas.
Important points about Hernia –
Inguinal hernias belong to ‘groin hernias’. In this group there are –
Femoral hernia – happens in femoral canal (not in inguinal canal)
Amyand’s hernia – the hernia sac is occupied by the vermiform appendix
Littre’s hernia – the hernia sac is occupied by the Meckel’s diverticulum
Classification of Hernia
- Direct and Indirect Inguinal hernias (explained above in detail)
- Reducible and Irreducible hernia:
Reducible hernia – This type of hernia can be pushed back into the abdomen by putting manual pressure to it
Irreducible hernia – This type of hernia cannot be pushed back into the abdomen by manual pressure. This is also called as incarcerated hernia.
Irreducible hernias are of 2 types:
Obstructed Hernia – In this the lumen of the herniated part of intestine is obstructed
Strangulated Hernia – In this, the blood supply of the hernia contents is cut off, thus leading to ischemia
Differential diagnosis
Femoral hernia – They occur just below the inguinal ligament when the abdominal contents pass through a naturally occurring weakness called the femoral canal. It appears as a bulge near the groin or thigh. The femoral canal usually allows the passage of femoral artery, smaller veins and nerves. It is seen commonly in women in comparison to men.
Epididymitis – is an inflammation of the epididymis, a tube near (behind) the testis which stores and carries sperms. It presents with pain and swelling in the testicles, along with pain, tenderness and or discomfort in the scrotum, epididymis or the testicles. Local inflammatory changes can also be seen. The diagnosis can be confirmed using Color Doppler Ultrasonography.
Testicular Torsion – occurs when the spermatic cord twists (when testicle rotates, twisting the spermatic cord that brings blood to the scrotum), cutting off the testicle’s blood supply, a condition called as ischaemia. The signs of torsion are extreme tenderness, rapid onset of pain in testicles, elevation of the testis, loss of landmarks, and absence of a cremasteric reflex. The diagnosis can be confirmed using Color Doppler Ultrasonography.
Lipomas – Liposarcoma; a rare fatty cancer is a deep seated tumor and most often grows on thigh, groin or back of the abdomen.
Inguinal adenopathy (Lymph node swelling) – is an enlargement of lymph nodes in the groin. It is usually caused either by infection or cancer
Saphena varix (Saphenous vein dilation) – is a dilation of the saphenous vein at its junction with the femoral vein in the groin. It presents with a bulge near the groin.
Pseudo-aneurysm (Vascular aneurysm) – It is also known as false aneurysm. It is the collection of the blood that forms between the 2 outer layers of an artery, the muscularis and adventitia. When this happens in the arteries around the groin (femoral artery and its branches), it causes a bulge which looks like hernia.
Hydrocele or Hydrocoele – is a term given to explain a ‘pathological accumulation of serous fluid’ in a body cavity. It can happen in any body cavity. But when this happens around the testis, it is called ‘Hydrocele Testis’. It is a condition in which there is accumulation of fluids around a testicle (cavities around the testicle). It is often caused by the fluid secteted by tunica vaginalis, one of the covering layers of the testis. (Tunica Vaginalis is a remnant piece of peritoneum wrapped around the testicle). Hydroceles occuring in kids below the age of 1 year usually resolve spontaneously if there is no hernia associated with hydrocele.
Varicocele – It is an abnormal enlargement of the pampiniform venous plexus in the scrotum (this plexus drains the testicles). It may develop as a result of poorly functioning valves that are normally found in veins. In other cases, it may occur from compression of a vein by a nearby structure. This can lead to decreased sperm production and quality leading to infertility. Palpation of enlarged veins during Valsalva maneuver is diagnostic on physical exam. Physical exam is diagnostic, but color Doppler ultrasonography can be used for confirmation.
Crypto-orchidism (un-descended testis) – It is a condition which presents with absence of one or both testes from the scrotum. It is the most common birth defect of the male genitals.
Pathophysiology
Indirect hernias, in men have the same route as that of the descending testes. The testis migrates from the abdomen into the scrotum during the developmental phase of urinary and reproductive organs. The larger size of the inguinal canal may be one reason for men to have inguinal hernia more than women (25 times more).
In normal individuals, strength of the posterior wall of the inguinal canal and shutter mechanisms compensating for raised intra-abdominal pressure prevent the hernia formation.
Management
Conservative management
Hernia truss – are used with an intention of contain a reducible hernia within the abdomen. It doesn’t cure the condition. If the pads are hard and intrude the hernia aperture they may scar or enlarge the aperture. Many trusses (old designs) can’t contain the hernia as their pads don’t remain in contact with hernia permanently. The modern varieties are made with non-intrusive flat pads. They come with a guarantee to hold the hernia securely during various activities throughout the day. Proofs have not been given that they could prevent progression of hernia. Truss can cause complications like strangulation, atrophy of spermatic cord and fascial margins. This further enhances enlargement of canal, making further repair difficult. It is a good choice and has been in demand for small painless hernias which could delay surgery or postpone it.
Elasticised pants – used by athletes, provide useful support as far as smaller hernia are concerned
Surgical management
Surgical correction of hernias is called as ‘hernia repair’.
It is generally not recommended in hernias having minimum symptoms. Surgery is associated with a risk known as ‘post herniorraphy pain syndrome’. Therefore in mild cases of hernia, ‘watchful waiting’ is advised keeping in view this painful syndrome.
Surgery is usually carried out as an ‘outpatient surgery’.
Surgical strategies to be considered in planning ‘inguinal hernia repair’ –
- Considering Mesh use – whether to use synthetic or biologic mesh
- Open repair
- Use of laparoscopy
- Type of anesthesia to be used – general or local anesthesia
- Appropriateness of bilateral repair etc
Laparoscopic surgery is generally considered for non-emergency cases
Minimal invasive open repair may have a lower incidence of post-operative nausea and mesh-associated pain.
Surgical correction is always recommended for inguinal hernias of childhood
Epidemiology
Direct inguinal hernia is less common (25-30 % of inguinal hernias). They usually occur in men over 40 years of age.
At some time in their life, about 27% males and 3% females develop a groin hernia or inguinal hernia.
Most often they occur before 1 year of age and also after 50 years of age.
In 2013 around 51,000 deaths and in 1990 55,000 deaths have been reportedly recorded due to inguinal, femoral and abdominal hernias.
Click to Consult Dr Raghuram Y.S. MD (Ayu)