

By Dr Raghuram Y.S. MD (Ay).
Have you ever seen anybody complaining of pain, numbness and weakness in the hand? Have you ever seen anyone who is squeezing their hands frequently after doing some work like lifting books, luggage or typing on their computer? Well, they might be suffering from a medical condition called ‘Carpal Tunnel Syndrome’
Table of Contents
What is Carpal Tunnel Syndrome?
Understanding the disease:
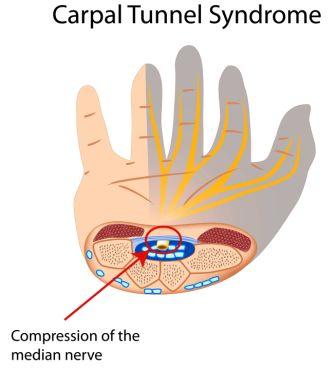
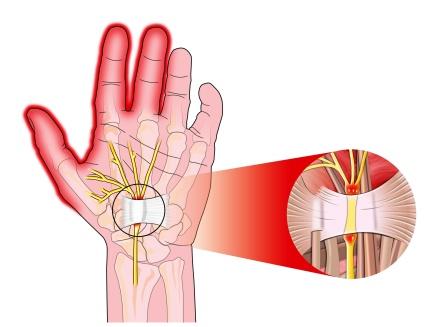
Carpal Tunnel Syndrome (CTS) is a medical condition presenting with pain, weakness, tingling sensation and other symptoms of discomfort in the hand. It is mainly caused due to the pressure on the Median Nerve in the wrist.
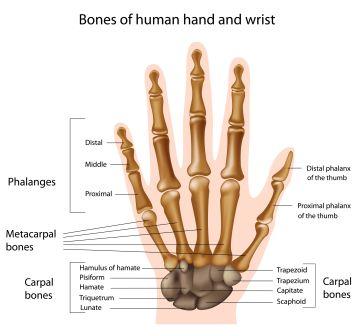
Carpal / Carpals: Carpal bones are the bones which make up the wrist. They are small bones of our hand and make up the Carpus (Carpus in Latin and Karpos in Greek means wrist). Carpals are 8 in number in each hand. Carpus connects the forearm to the hand through ligaments (cord like connecting tissues connecting one bone to the other) and some soft tissues. The free movements at the wrist are achieved by the mobility of individual carpal bones.
Carpal Tunnel (Carpal Canal): It is a narrow passageway on the palmar side of the wrist (side on which the nails are not seen). It is made up of bones and connective tissue. The Median nerve and many tendons pass through this canal. 9 flexor tendons (tendons of flexor muscles i.e. muscles whose contraction bends a joint) pass through the Carpal Tunnel. When one or more of these tendons swell or degenerate the canal further gets narrowed. The Median nerve gets compressed or entrapped as a result of narrowing of the canal. This causes Carpal Tunnel Syndrome.
Syndrome: Group of symptoms
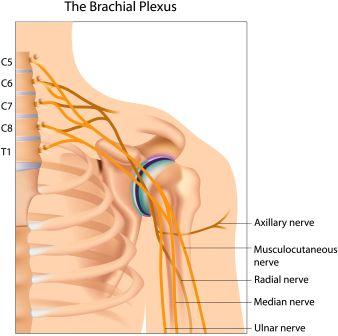
Median Nerve: It is one of the 5 main nerves taking their origin from the Brachial Plexus (Group of nerves starting from the lower part of the neck which in turn give rise to many nerves which control the sensation and movements of the muscles of arm, forearm and hand). Median nerve starts from cubital fossa (a depression at the junction of the arm and forearm) supplies and controls movement and sensation (feelings) of the forearm and hand (thumb and first 3 fingers, not little finger).
CTS is a condition in which Median Nerve which controls movement and sensation of the forearm and hand gets entrapped or compressed – due to the narrowing of Carpal Tunnel, due to swelling or degeneration of one of the tendons passing through the tunnel. This compression of median nerve leads to symptoms like pain, tingling sensation and numbness of the hand and fingers. The symptoms are experienced in the part of hand that is supplied by the median nerve.

Extension of Pain: The pain extends upwards to the arm. The discomfort also extends to the shoulder and forearm.
Symptoms
How should I know that I have CTS for sure?
- You will have tingling (feel of moving of ants), numbness, weakness and / or pain in the fingers of your hand (thumb, index finger, middle finger and half of the ring finger) but your little finger is fine
- You may find the symptoms in the forearm (portion between your hand / wrist and elbow)
- You may first note the symptoms at night. Even in the later period you will experience the symptoms predominantly while sleeping during night. The symptoms typically make you wake up from the sleep as the condition progresses.
- You may be able to get some relief by shaking or jerking your hands
What may my doctor look for when I go with symptoms resembling that of CTS?
- Your doctor would ask you more details about your tingling, numbness and pain, the time at which it is worst and what would you do to relieve it?
- The doctor will be interested to know if you have any health issues like arthritis, hypothyroidism or diabetes mellitus from a long time. He also wants to confirm if you are a pregnant.
- Doctor will try to know if you have hurt your wrist, arm or neck due to any reason in recent time
- The doctor will also try to know about your daily routine activities which could have hurt your wrist
- While examining you, the doctor will look for the feeling and strength in your hand, fingers, wrist and forearm. He will be conducting a few tests to confirm the diagnosis. He or she will also try to elicit the appearance of your neck, shoulders, arms, wrists and hands. Comparing the strength of both hands too will be done
- Hand diagram – The doctor may ask you to help fill in a diagram of hand to show where exactly you have symptoms
- For further confirmation, your doctor would advise you to undergo a few tests including blood test, nerve test, ultrasound, MRI etc
How do I manage with the symptoms in earlier condition?
When the symptoms are few you can manage them at home(Caution: Don’t try when the symptoms get worse)
- Stop any activity that causes numbness and pain
- Provide good rest for your wrists in between activities
- Soothe your wrists with ice-packs for 10-15 minutes once in every 2-3 hours
- To relieve pain and reduce swelling NSAID’s (Non steroidal anti-inflammatory Drugs) can be taken
- You can try wearing a wrist splint at night.
Note: Start the treatment and self care as soon as possible to stop the advancement of symptoms and to prevent the nerve damage
What should I do when home-level approaches of self-care don’t work out?
- See a doctor
- You also will need medicine for CTS and also for the disease at its backdrop (the disease which has caused CTS to occur)
- Surgery is the best option when many conservative methods and attempts to heal the symptoms fail and even after several weeks to months of other treatment
How can I prevent the recurrence of CTS once it is gone?
Health and lifestyle management
- Take care of your basic health, eat good food and live good life.
- Maintain body weight to normal proportions (corresponding to your BMI)
- Do not smoke or take alcohol
- Keep doing regular exercise to keep yourself strong, fit and flexible
- Keep taking medication and medical advises to get rid of your long-term diseases like diabetes, arthritis etc and keep them under good control
Wrist care
- Try keeping your wrist in neutral position
- Use the whole hand to hold and lift the objects rather than using only fingers
- When you are using the typing pad of your computer try keeping your wrists straight with the rest of your upper limb placed a little higher than the position of your wrists
- When you are doing repeated movements try to switch the movements or activities between both hands
Can there be improvement in CTS symptoms?
The symptoms of CTS usually develop gradually,
Symptoms often improve if you stop or change an activity that causes CTS
Most mild cases of CTS get better with self care (early care) and with slight treatment. Usually there is no permanent damage to the median nerve.

Symptoms of CTS improve by themselves when:
- Fluid build up in the body decreases (as it happens after pregnancy)
- When you stop or change the activity which has caused CTS
- Other health problems / diseases like obesity, diabetes etc. that cause or contribute to CTS improve
When to call for a doctor?
Call a doctor without delay or seek an appointment:
- If you notice sudden loss of sensation in your arm (upper limb)
- If you have tingling, numbness, weakness or pain in your fingers or hand that keeps coming again and again or if those symptoms have not responded for 2 weeks of home treatment
- If you have gradually developed little or no feeling in your fingers or hand
- If you are not able to do simple hand movements
- If you tend to accidentally drop the things from your hand (loss of grip)
- If you cannot pinch your thumb and index fingers together or if your pinch is weak
- If you cannot use your thumb normally (diminished thumb strength)
Ayurvedic tips for CTS
Ayurvedic tips for Carpel tunnel syndrome:
Apply Mahanarayana taila (herbal oil, available in any Ayurveda store. ). You can apply this two times a day.
After applying, do gentle wrist movements for 3 minutes.
After this, some heat therapy is very good.
You can do heat therapy
– by washing the wrist with hot water
– dipping a towel in hot water and fomenting the wrists with the towel.
– take castor leaves or Moringa leaves or both in a cloth. Tie it into poultice. Heat it over a pan and apply the poultice gently over the wrists.
– take crystal salt in a cloth, tie it into a packet. heat it on a pan. Apply the packet gently over the wrists.
Prevention:
Avoiding repetitive stress
Use correct postures or wrist and hand.
Work modification (Activity adjustment):
Use of ergonomic equipment like wrist rest, mouse pad etc
Take frequent breaks from activities to rest, stretch, change positions or alternate with another activity
Using alternatives to keyboard like digital pen, dictation, voice recognition etc
Change activities in which you make repeated finger, hand or wrist movements
Train yourself to use other positions or techniques that won’t stress your hand or wrist.
Arrange your activities and work space (workstation setup) using ergonomic guidelines (Workstation setup includes placement of your desk, computer monitor, paperwork, and chair and associated tools like computer keyboard and mouse etc)
- Speak to your HRD: If you feel that certain activities are causing numbness or pain in your fingers, hand or wrist you have to talk to your human resources department and ask about different ways or alternate options of doing your job, changes in equipment and other job assignments
- Avoid activities which stress your wrist like driving, working with small instruments, knitting, using vibrating instruments etc
- Wrist splint: Wear a wrist splint when you can’t control your wrist motion, such as while you are sleeping. Splint keeps your wrist in a neutral position (not bent too forward or backwards) and reduces the stress on your fingers, hand and wrist
- Control other health conditions such as arthritis, diabetes etc
- Restrict your salt intake – This tends to maintain fluid levels in the body
Note: There is no strong data or proof to support that activity adjustment or avoiding certain activities or work can prevent CTS because factors such as genetic predisposition and anthropometric features have stronger association with CTS as causal factors than occupational or environmental factors (such as repetitive hand use and stressful manual work)
Stage wise symptoms
Mild CTS symptoms: affect the hand and sometimes the forearm. They can also ascend up to the shoulder. Symptoms include:
- Numbness (Loss of sensation or less sensation)
- Pain in your hand, forearm or wrist that wakens you at night
- Shaking or moving your fingers might ease the symptoms
- Occasional Tingling sensation and feeling of ‘pins and needles’ or ‘crawling ants’
Symptoms in progressing disease:
- Intermittent numbness (partial or total loss of feeling) of the thumb, index and middle fingers and also the radial (thumb) side of the ring finger, a condition described as ‘sleeping hand’
- Tingling sensation and feeling of ‘pins and needles’ or ‘crawling ants’
- Numbness or pain which worsens while you are using your hand or wrist, you will feel it when you grip your hand or bend (flex) your wrist
- Occasional pain in forearm (area between wrist and elbow)
- Early morning stiffness (catches) in the fingers
- Burning sensation (in the same areas of hand explained above)
- Nature of pain: Numbness to the severity of waking one from their sleep
- Most often the numbness occurs at night. This is due to sleep position – due to flexing of wrists or sleeping on one side.
- Relief: Shaking or moving / jerking hands, wearing a wrist splint, prevents flexion of wrist
Less specific symptoms:
- Pain in the hands, wrists
- Loss of strength of grip
- Loss of manual dexterity – ability to make coordinated hand and finger movements to grasp and manipulate objects. Here, the person is not able to hold, grasp or manipulate objects.
Long standing / Chronic (Severe) CTS symptoms:
- Permanent nerve damage
- Constant numbness
- Weakness and Atrophy (waste away, degenerate, weaken) of some muscles of thenar eminence (bulge at the base of your thumb)
- Reduced strength and grip in the fingers, thumb or hand (loss of feeling and coordination in the fingers and hand)
You may accidentally drop your brush while combing or a spoon while eating
Loss of pinch strength: You will not be able to pinch an object between your thumb and first finger
You might not be able to do simple tasks involving your thumb like opening a jar or using a screwdriver because the thumb muscles would have got smaller and weaker (atrophy)
Weakness of pal-mar abduction (moving away from the body)
Note:
Symptoms of CTS often occurs in both hands but they are usually worse in one hand than the other
Not all pain in the wrist or hand is caused by CTS. Similar symptoms as those in CTS may be found when there is injury to the muscles, ligaments, tendons or bones, nerve damage in fingers, elbow or neck or in presence of arthritis in the wrist or joint of the thumb.
CTS is one of the most common causes of absence from work
Causes
- For most of the cases of CTS, the causes remain unknown
- The Aetiology of CTS is largely structural, genetic and biological with environmental and occupational factors such as repetitive hand use playing a minor and more debatable role. Thus CTS is an inherent, genetic, slowly but inevitably progressive idiopathic peripheral mononeuropathy. Related
- Anything that decreases the amount of space in the carpal tunnel, increases the amount of tissue in the tunnel or increases the sensitivity of the median nerve can lead to CTS. In short any cause or condition that can cause pressure on the median nerve might cause CTS
Risk factors
Predisposing / Secondary / Non-traumatic causes / Risk factors (Associated conditions):
Conditions or illnesses or associated diseases (local and systemic) which cause or contribute to arm (forearm) pain or swelling in the joints and soft tissues in the arm (forearm) or reduced blood flow to the hands can cause CTS. These are also called as risk factors.
Common conditions leading to CTS are:
- Obesity
- Hypothyroidism
- Diabetes, Pre-diabetes (Impaired glucose tolerance)
- Pregnancy
- Arthritis / Rheumatoid arthritis, Gout
- Lupus, Multiple sclerosis
- Down syndrome
- Amyloidosis
- Bad cholesterol
- Acromegaly
- Trauma
- Oral contraceptives
- Charcot-Marie-Tooth syndrome type 1 (Hereditary neuropathy)
- Factors which exert pressure from outside the canal: Benign tumours (Ex. Lipoma, Ganglion etc)
- Transthyretin amyloidosis associated polyneuropathy (Transthyretin amyloidosis deposition)
- Previous surgeries for carpal tunnel syndrome
Other risk factors:
- Being female (women between ages of 40 and 60 years)
- Women going through menopause or taking oestrogen
- Smoking – might cause CTS by affecting the blood flow to the median nerve
- Ageing – normal wear and tear of the tissues in the hand and wrist due to natural ageing process
Occupational causes:
CTS is a work-related disorder. CTS is often caused by such works and activities which require –
Forceful or repetitive hand movements
Repetitive or forceful movements at the wrist and hand (flexion and extension) – Means making the same hand movements repeatedly Ex. Bending down the wrist or making the same wrist movements again and again.
This might increase the fluid pressure in the tunnel through thickening of synovial tissues that line the tendons in the carpal tunnel and swelling of the membranes around the tendons (tenosynovitis).
- Hand-arm vibration
- Heavy manual works involving hand and arm viz working with vibrating tools
- Working for long periods in the same positions or awkward positions
Very High Risk Workers:
- Workers in the meat and fish packing industries
- Workers who assemble air-planes
- Automobile workers
- Musicians
Highest to Lowest Numbers of CTS Events by job (Ref: Published by Bureau of Labour Statistics, U.S. Department of Labour, November 2011):
- Cooks, institution, cafeteria
- Electrical power-line installers and repairers
- Painters, construction and maintenance
- Highway maintenance workers
- Welders, cutters, solderer’s and brazer’s
- Bus and truck mechanics and diesel engine specialists
- Construction
- Maids and housekeeping cleaners / Industrial machinery mechanics
- Labourers and freight, stock and material movers
- Automotive service technicians and mechanics
- Bus drivers, transit and intercity
- Maintenance and repair workers
- Telecommunications equipment installers and repairers, except line installers
- Janitors and cleaners, except maids and housekeeping cleaners / food preparation workers
- Truck drivers, heavy and tractor-trailer
- Heating, air conditioning and refrigeration mechanics and installers
- Truck drivers, light or delivery services
- Correctional officers and jailers
- Driver / sales workers / nursing aides, orderlies and attendants
- Carpenters
At home and play:
People who intensively cook, knit, sew, do needlepoint, play computer games, do carpentry or use power tools are at increased risk of CTS, Long distance cycling may worsen symptoms of CTS
Other causes:
- Hereditary causes
- Broken wrist bones, dislocated bones, new bone growth from healing bones, bone spurs – all these can block the tunnel and put sever pressure on the median nerve leading to the manifestation of CTS
- Carpal tunnel with a narrow diameter / size of Carpal tunnel
- Wrist-bones which are misaligned
- Certain habits like smoking
Non-traumatic causes for CTS:
Source
Non-traumatic causes happen over a period of time. Many of these factors are manifestations of ageing. Examples:
- Inflammatory diseases like Rheumatoid Arthritis etc. – These diseases cause inflammation of the flexor tendons causing pressure on median nerve in the carpal tunnel, leading to CTS.
- Diseases presenting with deposition of Mucoplysaccharides in the joints {like Hypothyroidism and Generalized Myxoedema} Mucopollysaccharides or Glycosaminoglycans are long chains of sugar carbohydrates. They are present in each and every cell –that help in building bone, cartilage, tendons, corneas, skin and connective tissue. They need to be broken on a regular basis by the action of lysosomal enzymes (11 in number). In diseases mentioned above, people do not produce one or more of the enzymes required to break down these sugar chains into simpler molecules (a condition called Mucopolysaccharidoses) or the enzymes which are produced do not work properly. Over a period of time these sugars collect in the cells, blood and connective tissues. This leads to permanent, progressive cellular damage which in turn affects the appearance, physical abilities, organ and system functioning and also the mental development of the person.
These sugars are also found in the fluid that lubricates our joints. In the diseases mentioned above, mucopolysaccharides get deposited in the perineurium of the median nerve and also the tendons passing through carpal tunnel. This brings in change of events leading to CTS.
- Pregnancy – Hormonal changes (High progesterone values) and water retention (causing swelling of synovium) during pregnancy predisposes to manifestation of CTS
- Previous injuries – Fractures of the wrist
- Disorders leading to fluid retention or associated with inflammation – Inflammatory arthritis, Colle’s fracture, Amyloidosis, Hypothyroidism, Diabetes Mellitus, Acromegaly, Use of corticosteroids and oestrogens
- Excessive production of growth hormones (in Acromegaly) – leads to the growth of soft tissues and bones around the carpal tunnel and compress the median nerve
- Tumours – Tumours such as ganglion or lipoma can reduce the carpal tunnel space by protruding into its space. This causes CTS (Rare cause)
- Obesity – In people classified as being obese (BMI > 29) become victims of CTS5 times more than thin individuals (BMI < 20)
- Double Crush Syndrome – There is a hypothesis which tells that compression or irritation of nerve branches contributing to median nerve in the neck or anywhere above the wrist joint, increases the sensitivity of the nerve to compression in the wrist. However this hypothesis is debatable.
- Genetic – one can get susceptible to neuropathy (disease or dysfunction of one or more peripheral nerves, typically causing numbness or weakness) including CTS when there is heterozygous mutations in the gene SH3TC2 associated with CMT (Charcot-Marie-Tooth disease – A genetically inherited disorder of peripheral nervous system characterized by progressive loss of muscle tissue and touch sensation across various parts of the body).
Diagnosis
Objective criteria: Electrodiagnostic testing (EMG and Nerve conduction velocity) to verify median nerve dysfunction
Supportive (subjective) criteria:
Clinical assessment by history taking and physical examination
Note: If clinical suspicion of CTS is high, treatment should be initiated despite normal electrodiagnostic testing. Source
Though there is no standard for the diagnosis of CTS, the below said are followed:
- Clinical findings (Thorough history and physical examination) including comparing the strength of both hands
- Subjective or supportive criteria – Recording the described symptoms
- Electrophysiology (Study of electrical properties of biological cells and tissues)
- Electrodiagnostic (EDX) testing {Measuring the speed and degree of electrical activity in muscles and nerves, common tests are EMG (Electromyography) and NCS (Nerve conduction Studies)} – This is said to be reliable and a confirmatory test. Median and Sensory nerve conduction studies provide a clinical diagnosis of CTS with 85% sensitivity and 95% specificity.
- Ultrasonography (Ultrasound) – To look at the size of the median nerve.
- MRI – To find the swelling in the median nerve, narrowing of the carpal tunnel or problems with circulation of blood through the carpal tunnel
- Blood tests: To check for a thyroid problem, diabetes or rheumatoid arthritis or any other medical problem associated with CTS
Role of MRI AND Ultrasound Imaging in the diagnosis of CTS is unclear
More about Electrodiagnosis:
When should electrodiagnosis be preferred in CTS?
There may be many conditions with similar symptoms like numbness, pain etc which may be misdiagnosed as CTS. Thus if the history and physical examination suggest CTS, we may go for electrodiagnosis with nerve conduction studies and electromyography (EMG)
Goal:
To compare the speed of conduction in the median nerve with the conduction in other nerves supplying the hand
When the median nerve is compressed as in CTS, it will conduct more slowly than normal. The conduction is also slow in comparison to the other nerves.
Options:
There are many EDX tests used for making a diagnosis of CTS
Among all these, the Combined Sensory Index (Robinson Index) is the most sensitive, specific and reliable test
What does it show?
Electrodiagnosis demonstrates impaired conduction across the carpal tunnel when the conduction is normal elsewhere in other nerves. Compression of the nerve results in the damage of myelin sheath of the median nerve and manifests in the form of delayed latencies and slowed conduction velocities.
Note: Normal Electrodiagnostic studies do not rule out the possibility of the presence of CTS. The disease pathology might not be established enough to give a positive result. CTS with normal EDX tests are very mild.
Diagnostic criteria for CTS (The American Association of Neuromuscular and Electrodiagnostic Medicine):
- Numbness in the distribution of Median nerve
- Nocturnal symptoms (symptoms like pain, numbness, tingling sensation flaring up at night)
- Weakness or atrophy of thenar muscles (bulge at the base of thumb)
- Positive Tinel’s sign at the carpal tunnel
- Abnormal sensory testing such as two-point discrimination
- Pain (less common than sensory disturbances)
Physical examination of patient
Provocative tests:
These are the physical manoeuvres which can be carried out in clinics for the confirmation of CTS. It needs little or no equipment.
Aim: The aim of the tests will be to temporarily increase the carpal tunnel pressure and provoke the symptoms of CTS.
Phalen’s test is said to be the oldest of these tests and still the best among the lot
These tests should be treated like any other medical investigation. They all generate some false positive results (abnormal results in subjects who do not have CTS) and some false negative results (normal test results in subjects with CTS)
If we carry out all of them aggressively in a given individual there is a high risk that at least one of them would produce a false positive result. The below mentioned are some of the Provocative tests which have been in use for the diagnosis of CTS over a period of time.
Phalen’s maneuver
The patient is asked to hold the affected forearm vertically (nails facing the ceiling of the roof) and support its elbow with another hand.
He is asked to flex (allow the wrist to drop) the wrist into 90 degrees under the influence of gravity (fingers pointing one of the wall and making 90 degree with forearm).
Forced flexion by the examiner (doctor) by grabbing the patients hand and deliberately bending it should be avoided as this may give false positive results
This test is safe to try at home in the presence of symptoms of CTS if done as described (optional). Anyhow don’t be curious until your doctor asks you to do it. Take care to note down the time within which the complaints occur.
The wrist is kept in that position for a couple of minutes
Positive for CTS: If the patient develops numbness in the area of median nerve distribution within 60 seconds he or she is said to have CTS
The quicker the numbness starts, the more advanced is the condition (The symptoms should be the same as the patient had experienced before conducting the test)
How it works? Phalen’s test works because wrist flexion elevates Carpal Tunnel pressure
Phalen’s sign – Pain or paresthesia in the fingers innervated by median nerve with one minute of wrist flexion
This test is positive in about 70% of cases
Reverse Phalen’s test
This is same as Phalen’s test but extension of wrist is tried instead of flexion in this case. The patient is asked to bend the wrist in the opposite direction (backwards) and keep it in position for a couple of minutes. The wrist is extended by 90 degrees in this case.
Positive for CTS:
When the symptoms as described the patient occurs after this manoeuvre he or she is positive for CTS. Even in extension the carpal tunnel pressure increases.
Limitations: This test is less studied than Phalen’s test. It is probably slightly less sensitive.
Tinel’s sign
The skin over the flexor retinaculum (a fibrous band on the Palmer side of the hand near the wrist, arches over the carpal bones of the hand, covering them forming the carpal tunnel) is lightly tapped to elicit a sensation of tingling or ‘pins and needles’ in the areas of median nerve distribution. Tapping is done with the physician’s finger or a tendon hammer.
Positive for CTS:
Pain and / or parasthesia (tingling, pricking, burning sensation) of the fingers innervated by the median nerve with percussion (tapping with fingers) over the median nerve suggests that the patient has CTS. The test is less sensitive, but slightly more specific than Phalen’s sign
Durkan test (Carpal compression test)
Apply firm pressure to the palm over the nerve up to 30 seconds
Positive for CTS: If the patient has CTS this test will induce pain and numbness along the areas distributed by median nerve
Hand Elevation Test
The patient’s hands should be held above the head for 2 minutes
Positive for CTS:
If the patient develops the same symptoms which he was complaining (numbness and pain in the median nerve innervated areas of wrist) then he is positive for CTS
Importance:
This is said to have higher sensitivity and specificity in comparison to Tinel’s test, Phalen’s test and Carpal compression test. This test originally showed 75% sensitivity and 98% specificity for CTS. This test has not been subjected to extensive studies
Tourniquet Test
A blood pressure cuff would be applied to either the upper arm or forearm, inflated between systolic and diastolic pressure. This is a less reliable test.
Positive for CTS:
The inflated cuff obstructs the venous return from the arm. The resulting increased blood volume in the hand increases the pressure in the carpal tunnel. If the symptoms as explained by the patient before the test appear, he or she is said to have CTS.
Flick Sign
This is not a provocative test like the above said tests.
The patient is asked ‘What do you do when you have the symptoms at night?’
If the patient demonstrates a ‘shaking out’ movement of flicking the wrists then the sign is positive for CTS.
Limitations:
Originally it was claimed to show 93% sensitivity and 95% specificity for CTS. Subsequently it has found to perform less well as confirmatory test.
Note:
A patient with true Carpal Tunnel Syndrome will not have any sensory loss over the thenar eminence (bulge of muscles in the palm of the hand and at the base of the thumb).
Reason: The palmar branch of the median nerve which innervates that area of the palm (thenar eminence) branches off the median nerve and passes over the carpal tunnel.
How to rule out CTS?
CTS are diagnosed in anyone presenting with pain, numbness, swelling and / or burning sensation in the radial side of the hands and / or wrists. When the pain is a predominant symptom it would not be a case of CTS (not a cause or source of symptoms).
Trigger point theories are not accepted by the current medical system because of deficit scientific evidence in support of their effectiveness.
Exercises for persons at risk of developing CTS:
- Isometric exercises: Example – Clinching the fist tightly, releasing and fanning the fingers out etc
- Stretches: Stretching the wrist before and after activity, between breaks is recommended. This will ease the wrist tension and relax it. The hand can be placed on a flat surface and gently pressed for a few seconds so as to stretch the wrist and the fingers
Allopathic treatment
Allopathic treatment for Carpal Tunnel Syndrome:
Goal of treatment of CTS:
- To allow you to return to your normal function and activities
- To prevent nerve damage
- To prevent loss of muscle strength in your fingers and hand
Physiotherapy (Physical Therapy)
- Proposed and recommended by American Academy of Orthopaedic Surgeons
- It is said to reverse pathology inside the carpal tunnel
- Any physiotherapy like myofascial release may take weeks of persistence application to effectively manage CTS
Non steroidal anti-inflammatory drugs (NSAID’s): Relieves pain and inflammation, relieves inflammation of tendon
Steroids (injected or oral)
- Corticosteroid injections can provide temporary relief but the patient has to go for lifestyle changes. Treatment with steroids is not recommended for extended periods. Steroids can be stopped once other treatment options are identified.
- Used when NSAID’s don’t provide good relief from pain and inflammation
- Corticosteroids are not used until nonsurgical treatments like rest, ice, splints, NSAID’s have provided no improvement in spite of using for several weeks
- They provide temporary relief; injected corticosteroids usually provide long-lasting results then oral steroids. But both rarely provide permanent relief.
Splinting:
- Indicated for light and moderate pathology (Non-invasive treatment at the beginning as recommended by the American Academy of Neurology)
- Wearing braces at night and also during such activities which cause stress on the wrists is highly recommended
(Night splints and corticosteroid injections are considered as conservative treatments)
Disease modifying treatment: Surgical release of transverse carpal ligament
Ultrasound therapy, Yoga, Acupuncture, Manual therapies such as mobilization
Laser treatment, Vitamin B6, Exercise therapy
Medicines (Corticosteroid or NSAID’s) should be used with other measures like ice, rest, splints etc for effective reception of pain and inflammation
When is surgery indicated?
The American Academy of Orthopaedic Surgeons recommends a course of non-surgical therapies before going for release surgery
Doctors consider surgery when
When the current treatment fails in giving a good relief within a time span of 2 to 7 weeks – alternate methods of treatment or surgery should be considered
Symptoms have not improved after several weeks to months of nonsurgical treatment (symptoms without signs of nerve damage). Nerve damage would make surgery more urgent
Symptoms restricting normal daily activities:
- Persistent loss of feeling or coordination in the fingers or hand
- Decreased strength in the thumb
- Sleep severely disturbed by pain
- Damage to median nerve (shown by nerve test results) and loss of hand, thumb or finger function
Early surgery with carpal tunnel release is suggested in below said conditions:
- Denervation of median nerve
- Patient electing to go for surgical treatment
Surgery (Carpal tunnel release surgery) –
It is a method in which the transverse carpal ligament is released by cutting the ligament. It relieves the pressure on the median nerve in the wrist.
Exercises for CTS, Videos
Wrist exercises to prevent CTS:
- Spiders doing the push-ups on a Mirror
How to do?
- Stand with your hands together in prayer position
- Spread fingers apart as far as you can. Then steeple the fingers by separating the palms of the hands while keeping the fingers together.
Benefits: This exercise stretches the palmar fascia, carpal tunnel structures and median nerve, relieves complaints of CTS
- The Shake:
How to do?
- Shake your hands like you have just washed them and are trying to dry them in air
- Do this for a minute or two once in every hour
Benefits: the flexor muscles and its median nerve can be prevented from getting tight and cramped throughout the day.
- Stretch Armstrong:
- Place one arm straight out in front of you, elbow straight, with your wrist extended and fingers facing the floor
- Spread your fingers slightly and use your other hand to apply gentle pressure to down-facing hand, stretching your wrist and fingers as far as you are able to do
- When you reach your maximum point of flexibility, hold this position for about 20 seconds
- Switch hands and repeat the exercise
- Do this 2-3 times on each side, hourly once if possible.
- Prayer stretch:
How to do?
- Place your palms together in front of your chest just below your chin
- Slowly lower your hands toward your waistline, keeping your hands close to your stomach and your palms together, until you feel a mild to moderate stretch under your forearms
- Hold for at least 15 to 30 seconds. Repeat 2-4 times in a day
- Wrist flexor stretch:
- Extend your arm in front of you with your palm up
- Bend your wrist, pointing your hand toward the floor
- With your other hand, gently bend your wrist farther until you feel a mild to moderate stretch in your forearm
- Hold for at least 15-30 seconds. Repeat 2-4 times in a day
- Wrist Extensor Stretch:
- Extend your arm in front of you with your palm down
- Bend your wrist, pointing your hand toward the floor
- With your other hand, gently bend your wrist farther until you feel a mild to moderate stretch in your forearm
- Hold for at least 15-30 seconds. Repeat at least 2-4 times a day. Source
- Fist and slide:
- Make a fist
- Slide your fingers upward until they are pointing up straight
- Repeat 5-10 times. Do it 2-4 times a day
- Fist and fan:
How to do?
- Make a fist
- Release your hand and fan out your fingers stretching them as far as possible
- Repeat 5-10 times. Do it 2-4 times a day.
- Read related – here and here
Limitations of Exercises in CTS:
- When used alone CT exercises aren’t likely to relieve symptoms
- Nerve gliding exercises can help the median nerve to move normally but sometimes can worsen symptoms
- If a median nerve remains trapped, nerve gliding exercises can stretch, irritate or injure the nerve
- CT exercises may be beneficial for mild to moderate symptoms when combined with other treatments such as modification, wrist splinting. Source
Few videos for CT exercises:
Massage for CTS:
Prognosis:
- CTS relieved after conservative or surgical management leaves minimal residue or nerve damage
- Long term CTS seen in elderly can result in permanent nerve damage i.e. irreversible numbness, muscle wasting and weakness
- Those who undergo carpal tunnel release are likely to develop trigger thumb in the months following the procedure. The chances are twice in comparison to those who haven’t undergone surgery.
Recurrence of symptoms after surgery is rare. Hand pain persisting after surgery might not have been caused by CTS. It may be due to inappropriate diagnosis.
Epidemiology:
- CTS can affect anyone
- It accounts to about 90% of all nerve compression syndromes
- 1 out of 20 people in USA suffer from the effects of CTS
- Caucasians have the highest risk of CTS compared with other races such as non-white South Africans
- Women (between ages 45-60 years) suffer from CTS 3 times more than men (3:1)
- Only 10% of reported cases of CTS are younger than 30 years of age
- Increasing age is a risk factor for CTS
- CTS is very common during pregnancy
Differential Diagnosis
Diseases which resemble CTS in presentation:
Osteoarthritis of the first carpometacarpal joint – Often seen associated with and coexisting with CTS
Signs: Painful stiff thumb joint, often worse in the evening
EMG: usually normal (unless CTS co-exists)
Stroke, acute:
Signs: Sensory and motor loss in a cortical type pattern i.e. whole hand or limb, worse distally or spinal segmental pattern. Ipsilateral (same side of the body) face and or leg may also be affected
EMG: completely normal peripheral nervous system
MRI or CT scan – show abnormalities in CNS (brain or spinal cord)
C6 Radiculopathy:
Signs: Sudden onset of severe unilateral neck pain radiating to shoulder / arm. Associated with weakness (shoulder movements and elbow flexion) and numbness predominantly of the dorsal aspect of 1st and 2nd fingers and lateral aspect of forearm
EMG: Normal Median nerve studies
MRI of cervical spine: Abnormality such as herniated disc or osteophyte impinging on C6 nerve root
C7 Radiculopathy:
Signs: Sudden of severe unilateral neck pain radiating to shoulder / arm. Associated weakness (mainly elbow, wrist, and finger extensors) and numbness predominantly of dorsal aspect of 3rd finger
EMG: Normal median nerve studies
MRI of cervical spine: Abnormality such as a herniated disc or osteophyte impinging on the C7 nerve root
Ulnar Neuropathy:
Signs: Sensory symptoms are on the medial aspect of the hand, distal forearm and 4th and 5th fingers. Abduction of 1st dorsal interosseous and 5th abductor minimi is weak. There is no weakness of the thumb.
EMG: Normal median nerve studies, abnormalities in ulnar nerve
Amyotrophic lateral sclerosis / Motor neuron disease
Signs: Widespread weakness and atrophy of muscle, progressive, fasciculations are prominent
EMG: Normal sensory nerves
De Quervain’s tenosynovitis:
Signs: Pain on movement of thumb and or wrist, commonly occurs in both wrists and worsens on heavy lifting, Hardening and thickening of the radial styloid may be indicative
EMG: Normal
Lateral epicondylitis:
Signs: Pain in the lateral elbow and lateral forearm, due to over-use (e.g. tennis), tenderness around the lateral epicondyle, may be associated with CTS
EMG: Normal (unless associated with CTS)
Rotator cuff tendonitis:
Signs: pain associated with arm movement, especially reaching, pain in the shoulder at night, tenderness on palpation around the shoulder, may be associated with CTS
EMG: Normal (unless associated with CTS)
MRI: Inflammation and exclude a tear in the rotator cuff
Polyneuropathy:
Signs: Symmetrical stocking and glove loss of sensation (worse in the feet) with or without mild weakness distally, distal reflexes are reduced or absent. It worsens pre-existing entrapment neuropathies (CTS in particular)
EMG: Widespread symmetrical, length dependent neuropathic changes without focal abnormalities in the median nerve across the wrist segment
Brachial plexopathies:
Signs: more widespread motor and sensory symptoms and signs beyond median nerve territory. True neurogenic thoracic outlet syndrome causes weakness in a median nerve territory. The sensory loss however is in the medial forearm, hand and fingers.
EMG: widespread neuropathy in a truncal, cordal or mixed patterns
MRI: Increased signal intensity in parts of plexus and in denervated muscles. Cervical spine and cord is usually normal
Proximal median neuropathies:
Signs: Numbness extends across the thenar eminence (palmar branch) and weakness includes forearm pronation and wrist flexion
EMG: Neuropathic changes in the palmar branch of the median nerve
Multiple Sclerosis:
Signs: sensory/motor loss may vary over time and place.
EMG: Normal peripheral nervous system
MRI or CT scan: abnormalities in CNS (brain and spinal cord)
Guyon Canal Syndrome (Ulnar tunnel syndrome):
Signs: Loss of sensation in the ring and little finger and in the outer half of the palm, associated with CTS
Source
Digital Flexor Tenosynovitis (Trigger or Snapping Finger):
Signs: Pain and clicking sound when the trigger finger or thumb is bent and straightened, common in people with hypothyroidism, diabetes, gout, rheumatoid arthritis or connective tissue disorders
Thoracic outlet syndrome:
Signs: Symptoms similar to CTS, Raynaud’s phenomenon (changes in sensation and temperature in the hand)
Source
CTS and Ayurveda
We cannot coin or plug any single disease explained in Ayurveda with Carpal Tunnel Syndrome. Rather we do not have any straight reference of a disease in Ayurveda which matches with the clinical presentation of CTS explained and found in modern day medical science and practise.
We can assemble a few conditions explained in Ayurveda and try to make a close comparison to CTS
The below said diseases, symptoms or conditions explained in Ayurveda fall in close proximity of the clinical picture of CTS
Vatarakta / Vatashonita
This term is generally associated and compared to Gout or Rheumatoid Arthritis. It is also compared to peripheral vascular diseases. The contaminated Vayu and rakta (blood) get amalgamated together and jointly produce a disease called Vatarakta or Vatashonita.
Among the sites of manifestation of Vatashonita it is said:
तस्य स्थानं करौपादावङ्गुल्यः सर्वसन्धयः।
कृत्वाऽऽदौ हस्तपादे तु मूलं देहे विधावति॥{च.चि.२९/१२}
tasya sthānaṃ karaupādāvaṅgulyaḥ sarvasandhayaḥ|
kṛtvā”dau hastapāde tu mūlaṃ dehe vidhāvati||{ca.ci.29/12}
Vatashonita is a disease manifested in the hands, foot, fingers and toes of the extremities and all the joints of the body. It takes its origin from the root of hand and foot (wrist and ankle joints?) and gradually spreads all over the body. {Ref: Cha.Chi.29/12}
Since CTS too has its root in the carpal tunnel and is related with the fingers of the hand, Vatarakta specially manifested in the hand (wrist) and fingers or taking its origin in the karamula or wrist joint can be compared to CTS.
स्वेदोऽत्यर्थं न वा कार्ष्ण्यं स्पर्शाज्ञत्वं क्षतेऽतिरुक्।
सन्धिशैथिल्यमालस्यं सदनं पिडकोद्गमः॥
जानुजङ्गोरुकट्यंसहस्तपादाङ्गसन्धिषु।
निस्तोदः स्फुरणं भेदो गुरुत्वं सुप्तिरेव च॥
कण्डूः संधिषु रुग्भूत्वा भूत्वा नश्यति चासकृत्।
वैवर्ण्यं मण्डलोत्पत्तिर्वातासृक्पूर्वलक्षणम्॥{च.चि.२९/१६-१८}
svedo’tyarthaṃ na vā kārṣṇyaṃ sparśājñatvaṃ kṣate’tiruk|
sandhiśaithilyamālasyaṃ sadanaṃ piḍakodgamaḥ||
jānujaṅgorukaṭyaṃsahastapādāṅgasandhiṣu|
nistodaḥ sphuraṇaṃ bhedo gurutvaṃ suptireva ca||
kaṇḍūḥ saṃdhiṣu rugbhūtvā bhūtvā naśyati cāsakṛt|
vaivarṇyaṃ maṇḍalotpattirvātāsṛkpūrvalakṣaṇam||{ca.ci.29/16-18}
Sparshaagnatvam (Loss of sensation), Nistoda (Pricking pain), Bheda (splitting pain), Gurutva (heaviness) and Supti (Numbness / Paraesthsia) are some of the prodromal (premonitory) symptoms of Vatashonita which occurs in almost all the joints of the body including wrist joint and joints of the hand and fingers. These symptoms point towards the CTS. Thus CTS can be said to be a part of Vatashonita. CTS might occur during the pathogenesis of Vatashonita and also is a part of premonitory symptoms and symptom complex of Vatashonita.
Even in the modern medicine we can find the mention of gout and rheumatoid arthritis as the predisposing or associated or risk factor of CTS.
The below said symptoms explained in the subtypes of Vatashonita also point out towards CTS:
- Toda (pricking sensation – feeling of needles and pins) and shula (pain) in the wrist and joints of the hand and finger as explained in Vataja Vatashonita lakshanas (signs and symptoms of Vatashonita manifested by contamination of Vayu)
- Angulisandhinam sankocha – constriction / congestion of (around) the finger (hand) joints / wrist explained in Vataja Vatashonita lakshanas point towards narrowing of carpal tunnel and consequential median nerve irritation
- Vidaha (localised burning sensation) – mentioned in the context of Pittaja Vatashonita lakshanas (signs and symptoms of Vatashonita manifested by contamination of Pitta)
- Supti (Numbness, feeling of crawling ants) and Manda ruk (low intensity pain or less pain) mentioned in the context of Kaphaja Vatashonita lakshanas (Signs and symptoms of Vatashonita manifested by contamination of Kapha)
Vishvachi
Vishvachi is another condition whose explanation seems to be closer to the clinical picture of CTS
तलं प्रत्यङ्गुलीनां या कण्डरा बाहुपृष्ठतः।
बाह्वोः कर्मक्षयकरी विश्वाचीति हि सोच्यते॥ {यो.र.वा.व्या.७१}
talaṃ pratyaṅgulīnāṃ yā kaṇḍarā bāhupṛṣṭhataḥ|
bāhvoḥ karmakṣayakarī viśvācīti hi socyate|| {yo.ra.vā.vyā.71}
It is said about Vishvachi:
‘The condition in which the vitiated (contaminated) Vata afflicts the Kandaras (tendons / nerves) – which extend from the front of (palmar surface) the fingers and palm (wrist?) to the back (spine – backbone especially the scapular part of the upper back) – passing through the forearm and arm causing stiffness and rigidity of the same tendons leading to the destruction of the functions of the arm (upper limb including hands) is called Vishvachi’
In this explanation it is clear that the disease Vishvachi afflicts the tendons and nerves of the hand, wrist and fingers which bring it into the proximity of CTS.
Amavata
Amavata is a term which is used to describe a symptom complex in Ayurvedic pathology which resembles the disease Rheumatoid Arthritis of the modern day. Some experts have also seen it in comparison with Gout. The disease manifests in 2 different forms. The first form (stage) is moreover a systemic representation or manifestation of the early disease process when the joints, bones and soft tissues of the body have not yet been afflicted. The second form (stage) is a progressive / progressed stage of a disease (Pravridda Amavata) wherein we can find the disease manifesting in its full form with both of its systemic and local components.
The local components include the affliction of joints, bones and soft tissues. This stage also comes with its complications.
Amavata afflicting the wrist joint and fingers of the hand can be compared to CTS. Thus CTS can be included in Amavata afflicting the hand joints and fingers.
We also learn that Rheumatoid Arthritis is often associated with CTS in the form of a causative / predisposing or a risk factor
Avabahuka / Apabahuka
Avabahuka is a condition which cannot exactly be correlated with CTS but it can be considered into the context because Avabahuka too is a condition in which the whole upper limb is involved
शिराश्चाऽऽकुञ्च्य तत्रस्थे जनयत्यवबाहुकम्॥{यो.र.वा.व्या..८०}
śirāścā”kuñcya tatrasthe janayatyavabāhukam||{yo.ra.vā.vyā..80}
It is said about Avabahuka:
‘The morbid Vayu located in the upper limb causes a condition called Avabahuka by constricting the Sira’s (blood vessels, nerves and tendons) leading to the manifestation of symptoms like pain, numbness etc in the whole of the upper limb’
Other conditions
Similarly the below said conditions can be included under CTS:
Ekangavata: Vata vitiated in any part of the body afflicts that part and causes Ekanga vata. If the morbid vata / vayu is vitiated in the hand it can cause symptoms resembling CTS because the symptoms like pain, numbness, loss of movements, feeling of needles, pins and ants etc are generally caused by morbid vayu be it the whole body or a part of it. To be precise Ekanga vata in the hand can be the symptoms of CTS manifested due to the degeneration of tendons in the carpal tunnel leading to median nerve irritation.
Ekanga Roga: This is a condition which might be synonymous with Ekangavata explained above. We can find it mentioned in the ‘Asthapyaha’ category of patients i.e. the patients who are fit to receive medicated decoction enema (Cha.si.2/16)
Similarly the below said conditions which are explained in the Asthapya category can be considered to belong to the class of CTS:
- Panibhuta – Pain, numbness etc symptoms in the hand / palm / wrist
- Bahushoola – Pain, numbness etc in the arm / forearm
- Anguli shoola – Pain, numbness etc in the fingers, carpals etc
Ayurvedic treatment
By considering all the above mentioned conditions explained in Ayurveda around the vicinity of the clinical picture of CTS, the treatments mentioned for the same conditions in their respective contexts can be summed up as Ayurvedic treatment / medicinal options for CTS
Below given are some of the best options for an Ayurvedic management of CTS:
Preventive aspects:
Taking a well balanced diet and following a healthy and happy lifestyle so as to ‘keep in good balance’ all the 3 factors responsible for our health when in normal condition and for our illness when disturbed i.e. the Tridoshas – Vata, Pitta and Kapha. This also holds good for those prone to get CTS, those who have had a couple of attacks of CTS or those who have been treated for CTS. This also helps to check the progression of the disease in those who have an active disease in a progressive mood.
Vata can be kept at bay by not consuming foods which are not cold, dry, stale, rich in spices, bitter and astringent tastes, avoiding cold breeze, excessive sex, vigil and exercise, keeping away from anxiety, fear and stress, managing rainy season etc – This will prevent the further degeneration process of tendons and nerves.
Pitta can be checked by not consuming foods which are hot, spicy, rich in salt and sour tastes, avoiding excess exposure to heat and fire, keeping away from anger and extremes of emotion and stress, managing spring season and summer etc – This will prevent the further inflammation taking place in the joints, bones, soft tissues, tendons and nerves and help in recovery process.
Kapha can be managed by avoiding foods which are cold, oily, stale, refrigerated, heavy to digest, slimy, food rich in sweet, sour and salt taste, keeping away from low moods and depression, avoiding excess of sleep, lack of exercise and sex, sedentary life activities, managing cold season etc – This will prevent stagnation’s and blocks in the cells and tissues and thus prevent pressure on nerves and tendons
Nitya Abhyanga and Snana: Application of medicated oils daily and taking a relaxing shower will help. A soothing massage either done by self or with some help from family members would be handy. If it is not possible daily, it can be done on a ‘twice-a-week’ basis. Oil application can be given to the affected wrist or fingers once the symptoms become evident.
Pratimarsha Nasya: Nasal instillation of medicated oils in a small dose on a daily basis will strengthen the nerves and enhance the blood supply to the joints and soft tissues (wrist and fingers in this context). 2 drops of the medicine in each nostril will do wonders in CTS.
Curative approach:
External treatments:
The below said treatments are highly effective in CTS
Abhyanga:
Massage with medicated oils always provides a soothing effect and relieves pain, numbness, tingling sensation etc symptoms. Care should be taken not to give a vigorous massage so as to aggravate the conditions.
Abhyanga should be done under supervision of a qualified and experienced Ayurvedic doctor. Ayurvedic doctor might recommend oils or combination of oils and ghee (medicated) based on the predominance of Doshas for a better result.
Samvahana:
It is also a type of Abhyanga where in the affected part is given a fine wipe (light touch massage) or caressing after the application of medicated oils
Swedana:
Fomentation / heat / steaming / sweating is given using medicinal herbs. This will be handy when Vata and Kapha symptoms are involved.
When Vata symptoms like numbness, tingling sensation and pain are predominant – Swedana is given in the form of –
- Patra Pinda Sweda – Bolus fomentation with medicated leaves like Nirgundi (Vitex negundo), Eranda Patra (Castor – Ricinus communis leaves) etc
- Shashtika Shali Pinda Sweda – Fomentation with Shashtika rice processed in milk prepared with herbal decoctions. This treatment apart from healing property also has nutritive property.
- Bashpa Sweda / Nadi Sweda: Steam from herbal decoctions to the afflicted area after Abhyanga
- Sthanika Avagaha: Dipping the affected part in the herbal decoctions or processed milk.
- Parisheka Sweda: Spraying in of herbal decoctions etc on afflicted part
Note: Dashamula Kashayam, Dashamula sidda ksheera (milk processed with Dashamula decoction) is generally used for the purposes of Bashpa and Parisheka sweda and Sthanika Avagaha
Upanaha: Medicated poultices are tied and left in place for a few hours. Atasi Upanaha, Shalvana Upanaha,Tila Upanaha etc are some of the effective Upanaha’s used in CTS
When Kapha symptoms like stiffness, swelling, mild pain, numbness, tingling sensation etc are predominant – Swedana is given in the form of –
- Churna Pinda Sweda: Bolus fomentation with herbal powders made hot and applied on the afflicted part. Kottamchukkadi churnam, Grihadhoomadi churnam, Kolakulattadi churnam, Jatamayadi churnam, Rasnadi churnam etc are used for Churna Pinda Sweda.
- Valuka Sweda: Sand bolus fomentation especially if Rheumatoid arthritis is causing swelling and other symptoms of CTS
Other form of Sweda’s as mentioned in Vata related symptoms like Bashpa Sweda, Sthanika Upanaha, Parisheka and Upanaha can also be done as and when required
Note:
- Swedana should not be given in CTS predominant with Pitta and Rakta symptoms like burning sensation, inflammation, raised heat, redness around the afflicted joint, feeling of fumes coming out etc
- In these conditions it is always better to adapt Sheetala upachara’s / prakriya’s or cooling treatments like ice pack etc
Dhara: Pouring in stream of medicated oils and liquids on the afflicted parts
Kashaya Dhara – Stream pouring of herbal decoctions like Dashamula Kashaya etc
- Ksheera Dhara – Milk processed with Dashamula, Yashtimadhu, Laksha etc are poured over the afflicted part after giving an Abhyanga with medicated oils / ghee / oils + ghee
- Taila (Ghrita) Dhara: Medicated oils are poured over the afflicted part in streams. Taila can be made warm as in case of Vata and Kapha predominant symptoms. Taila’s like Pinda Taila, Yashtimadhu Taila etc can be used without heating in cases of Pitta and Rakta predominant conditions of CTS. Medicated ghee too is highly effective when used in Vata, Pitta or Rakta predominant conditions. A mixture of medicated ghee and oil (Yamaka) is also preferred in some conditions.
- Dhanyamla Dhara: Fermented medicated liquids called Dhanyamla or Kanji is used in case of presence of severe inflammatory symptoms in CTS, like a CTS developed on the backdrop or as a complication of Rheumatoid Arthritis
Lepa: Application of herbal pastes is called Lepa.
Paste can be prepared from the same Churna’s (powders) used in Churna Pinda Sweda i.e. Kottamchukkadi churnam, Grihadhoomadi churnam, Kolakulattadi churnam, Jatamayadi churnam, Rasnadi churnam etc
Bandhana: Bandaging the area either after application of some medicaments or just to provide support, this can be compared to the modern day concept of splinting
Greeva Vasti: Oil pooling in the region of cervical spine (bones of neck) is said to soothe the nerves of brachial plexus whose branches supply the whole upper limb including hand, wrist and fingers. The health of these nerves is essential for smooth functioning and feeling in the upper limb. This can be combined with Pinda Sweda and Nasya.
Oils and ghees
Oils and Ghee used for Abhyanga, Samvahana and Dhara:
- Ksheerabala Tailam
- Mahanarayana Tailam
- Mahamasha Tailam
- Dhanwantaram Tailam
- Cheriya Prasarani Tailam
- Valiya Prasarani Tailam
- Bala Tailam
- Bala Guluchyadi Tailam
- Yashtimadhu Tailam
- Murivenna
- Kottamchukkadi Tailam
- Pinda Tailam
- Tiktaka Ghritam
- Mahasneham etc
Internal treatments
Abhyantara Chikitsa (Internal Treatments):
Snehapana: (Oral intake of medicated ghee / oil / both):
Snehapana helps in healing the inflammatory process by the virtue of the properties of its medicines. If taken on a daily basis (Nitya Sneha Pana) in a low dose it helps in relieving the patient from symptoms of CTS like numbness, tingling sensation, pain etc. It soothes the nerve, improves blood circulation to the afflicted area, support’s bone and soft tissues.
The same medicines which are used for Nitya Snehapana can be used for Shodhana Sneha (for giving in larger doses before cleansing procedures like Virechana)
Some of the highly effective oils (tailam) and ghee (ghritam) which are used in Snehapana are:
- Guggulutikaka Ghrita
- Tiktaka Ghritam
- Kalyanaka Ghritam
- Rasnadi Ghritam
- Triphala Ghritam
- Ksheerabala tailam – 101
- Maharajaprasarani tailam / Mharajaprasarani tailam capsules
- Gandha Tailam / Gandha Tailam capsules
- Suddhabala Tailam etc
Virechana: Therapeutic purgation (giving herbal laxatives and purgatives), this too can be done in 2 different methods –
Krama Virechana – This is the therapeutic method of purgation wherein the whole process of Snehapana, Swedana and Virechana are followed in that chronological order within a stipulated time period of 7-15 days.
Nitya Virechana – Herbal laxatives are given on a daily basis
Note: Aim of Virechana is to keep eliminate the toxins from the body, gain control over the morbid Dosha’s, strengthen the tissues and reverse the disease process. The aim of Nitya Virechana is to keep flushing out the toxins and unnecessary metabolites which can damage the body tissues on a regular basis and in small quantities.
Medicines for Virechana
Effective medicines used for Virechana are:
- Gandharvahastadi Kashayam
- Sukumara Kashayam
- Pathyakshadhatryadi Kashayam
- Sukumara Ghritam
- Tiktaka Ghritam
- Trivrit Leham
- Sukumaraa Leham
- Mridvikadi Leham
- Avipatti Churnam etc.
Vasti treatment
Vasti: Medicated enemas are said to be the best treatments for controlling Vayu and thus tackling the other morbid factors in the body. Enemas not only help in cleansing in the bowel, they also set right the metabolism, soothe the nerves, flush the toxins, regularize the functions of all the tissues, gets rid of stress, helps recover from the diseases, prevent the recurrence of the diseases and provides immunity. Enemas are specially indicated in bone, joint and soft tissue injuries.
Enemas too can be given in different forms (choice is made on the type of morbidity and strength and constitution of the patient) –
Kashaya Vasti or Asthapana Vasti: Herbal decoctions are used in the form of enemas.
Ksheera Vasti: For those who do not tolerate the intensity and strength of Kashaya Vasti, Ksheera Vasti (milk medicated with the herbal decoctions) is preferred. Ksheera vasti is preferable in the inflammatory conditions and in predominance of pitta and rakta symptoms in CTS.
Sneha Vasti / Anuvasana Vasti: Enemas with herbal oils, can be used individually or in combination with Kashaya / kshera vasti, used predominantly in Vata and Pitta association in CTS (degenerative and inflammatory changes)
Matra Vasti: It is a variant of Anuvasana Vasti or Sneha Vasti. This enema is administered on a daily basis for the prescribed duration in small doses.
Some Important Vasti’s which are useful in CTS:
- Erandamuladi Kashaya Vasti
- Dashamula Kashaya Vasti
- Dashamula Ksheera Vasti
- Sneha / Anuvasana / Matra Vasti with Guggulutiktaka Ghritam
Nasya treatment
Nasya: Instillation of medicines (medicated oils, ghee, powders, etc) in the nose. Nose is said to be the door for the head and nervous system in Ayurveda. The medicines instilled in this method is said to soothe and strengthen the nerves, sense organs and all organs and tissues above the level of collar bone. This is found to be highly effective in CTS.
Important medicines used for Nasya:
- Anu tailam
- Shadbindu Tailam
- Ksheerabala Tailam 101
- Dhanwantaram Tailam 101
- Mahamasha Tailam
Ayurvedic medicines
Effective Ayurvedic medications for CTS:
Kashayam (herbal decoctions)
- Prasaranyadi Kashayam
- Punarnavadi Kashayam
- Gandharvahastadi Kashayam
- Rasnaerandadi Kashayam (Cheriya Rasnadi Kashayam)
- Maharasnadi Kashayam (Valiya Rasnadi Kashayam)
- Rasonadi Kashayam
- Kokilaksham Kashayam
- Guggulutiktakam Kashayam
- Balaguluchyadi Kashayam
- Pathyakshadhatryadi Kashayam
- Kokilaksham Kashayam
- Kalyanakam Kashayam
Asavas and Arishtas: (herbal fermented liquids)
Ghritam (medicated ghee)
- Varanadi Kashayam
- Guggulutiktakam Ghritam
- Tiktakam Ghritam
- Brahmi Ghritam
- Saraswatha Ghritam
- Kalyanaka Ghritam
Tailam and Avarta Tailam (medicated oils and fortified oils):
- Dhanwantarm tailam 101
- Ksheerabala tailam 101
- Shuddabala tailam
- Mahamasha tailam
- Maharajaprasarini Tailam
Churnam (Herbal powders):
- Ashwagandha Churnam
- Shatavari Churnam / Shatavaryadi Churnam
- Kapikachchu Churnam
- Bala Churnam
Leham and Rasayanam (Herbal confections, jams and rejuvenators):
- Chyawanaprasham
- Dashamula Haritaki Leham
- Ashwagandhadi Leham
- Vanari Kalpam
Guggulu and Vati (Guggulu preparations and tablets):
Click on the medicine names to learn more about them
- Kaishora Guggulu
- Simhanada Guggulu
- Yogaraja Guggulu
- Rasnadi Guggulu
- Mahayogaraja Guggulu
- Punarnavadi Guggulu
- Chandraprabha Vati
- Mahavatavidhwamsini Rasa
- Vatavidhwamsini Rasa
- Ekangaveera Rasa
- Brihat Vata Chintamani Rasa
- Valiya Marma Gulika
- Vayu Gulika
- Dhanwantaram Gulika
Single drugs useful in CTS:
Click on the herb names to know more about them
- Rasona (Garlic – Alium sativum)
- Ashwagandha (Withania somnifera)
- Bala (Sida cordifolia)
- Guggulu (Commiphora mukul)
- Punarnava (Boerhavia diffusa)
- Prasarini (Paederia foetida)
- Shatavari (Asparagus racemosus)
Research, facts
Research works and interesting facts about CTS
- According to the scientific data available from NIOSH (National Institute for Occupational Safety and Health), job tasks that involve highly repetitive manual acts or specific wrist postures were associated with incidents of CTS (causation was not established). A 2010 survey by NIOSH showed that 2/3 of the 5 million CTS cases in the US were related to work. Women have more work related CTS than men. Source
- Over expression of ‘Transforming growth factor-b’ (TGF-b) AND Connective tissue growth factor (CTGF) in the sub-synovial connective tissue (SSCT) is likely to be found in patients suffering from CTS. These 2 factors can lead to increased fibrosis in the SSCT of the carpal tunnel leading to narrowing of space and pressure on median nerve leading to CTS. Source
- Psycho-social factors in the workplace: Studies indicate that psycho-social factors in the workplace, such as intense deadlines, a poor social work environment, and low levels of job satisfaction are major contributors to CT pain. Source
- Studies show that the jobs in manufacturing industry are associated with an increased risk of work-related CTS
- Studies have shown that mental status parameters or alcohol use yields poorer overall results of treatment
- Square Wrists: Some studies have shown that the people who have square wrists (thickness and width are the same) have a greater risk of getting CTS in comparison to those with more common rectangular shape
- Palm Shape: according to one study, patients with palms that were both shorter and wider than average and who also had shorter third fingers, were more likely to have CTS than those without these hand characteristics
- Poor upper back strength: Some researchers claim that poor upper back strength makes people more susceptible to poor posture and injuries in the upper extremities, including carpal tunnel syndrome. Source
Important points about CTS
- CTS was most commonly heard in the years following World War II
- We can find the condition depicted in the mid 19th century surgical literatures
- In 1854, Sir James Paget was the first to report median nerve compression at the wrist in a distal radius fracture
- CTS was most commonly noted in medical literature in the early 20th century but the first use of the term was noted in 1939
- Physician Dr George S. Phalen of the Cleveland Clinic identified the pathology of CTS after working with a group of patients in the 1950’s and 1960’s
You have the best remedies for Carpal Tunnel Syndrome in Ayurveda but don’t forget to consult an Expert Ayurveda Doctor for an opinion before starting on with anything.



5 comments
Dipanjan
Is it proper to consume sour foods like SAMBHAR at night ?
aryambal
Seeing the Doctor. Taking medicines and physio therapy is very helpful. Oil-pulling accelerates the curing process to a large extent.
Rajalakshmi Gopalan
Your article on CTS throws immeasurable information ! Even a layman can easily understand the medical terms. Various ways to minimise the pain and endeavour to arrest further advancement explained serve as an eye opener particularly for the younger professional persons. I have read every word of this article and intend seeing the videos leisurely.
Dinakar Reddy
Hi Sir,
One of my cousin both hands little week now and figures bent slightly. After concern doctor and medical tests, doctors reported us that he got impacted with ‘Motor Neuro borderline neuropathy of Median and Alnar nerve’. Since 5 months he is having this problem.I would like to know that whether it can be completely curable or not and how complicate it is. Now he feel some shivering for his leg as well. Please provide your opinion as soon as possible.
Thanks,
Dinakar.
GEETA MATHEW
Doctor,
I have numbness in all fingers including little finger, especially at the tips. Is this related to CTS ? i had changed my dish washing soap and experienced a bit of skin peeling, & extreme dryness. And initially thought the numbness was due to that. But these symptoms are persisting tho i changed the soap.