Article by Dr Raghuram Y.S. MD (Ay)
Psoriasis is a medical challenge and has an autoimmune process at its backdrop, wherein your immune system which is supposed to protect you will be acting in a harmful way against your own body.
Similarly Arthritis is another condition which has been giving pain and crippling the mankind since ages and is posing a huge challenge to the medical system.
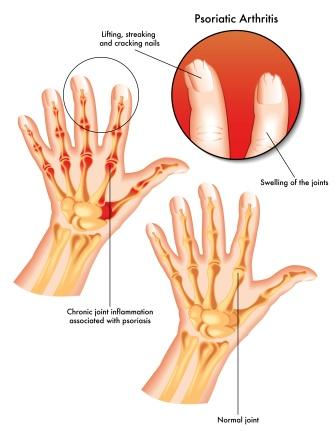
Table of Contents
Psoriatic Arthritis
Is a type of inflammatory arthritis. It is seen to develop in 6-42% of people who have the chronic skin condition called ‘Psoriasis’. It has been classified as a ‘sero-negative spondylo-arthropathy’
Other names:
Arthritis psoriatica
Arthropathic psoriasis
Psoriatic arthropathy

Signs and Symptoms
Pain, swelling or stiffness in one or more joints
Redness in the joints (inflammation)
Warmth in the joints (inflammation)
Asymmetrical oligo-arthritis – inflammation affecting one to four joints during first 6 months of the disease (70% cases), 15% of these arthritis is symmetrical
Joints involved – Proximal inter-phalangeal Joints (PIP), Distal Inter-Phalangeal Joints (DIP), Metacarpo-Phalangeal Joints (MCP) and Wrist joints. Involvement of DIP joints is a characteristic feature and is present in 15% cases.
Sacro-iliitis or spondylitis – pain in the sacral region (lower back, above the tailbone), in 40% cases
Enthesitis – pain can occur in and around the feet and ankles (especially enthesitis in the Achilles tendon or inflammation of the Achilles tendon where it inserts into the ankle bone)
Plantar fasciitis – pain in the sole of the foot
Arthritis mutilans – complication of severe arthritis presenting as a ‘pencil-in-cup’ appearance on X-ray
Joint damage – due to prolonged inflammation
Psoriatic arthritis may also affect fingers, nails and skin
Dactylitis – sausage like swelling in fingers or toes
Nail changes – pitting or separation of nails from the nail bed, onycholysis, hyperkeratosis under the nails, horizontal ridging of nails

Psoriasis – Scaly skin lesions which are most common over the extensor surfaces such as scalp, natal cleft and umbilicus
Extreme exhaustion – will be present along with pain and inflammation. This exhaustion will not go away in spite of adequate rest.
Note:
Psoriatic arthritis either remains mild or may progress to manifest as a destructive disease of joints.
Periods of active disease or flares will alternate with periods of remission.
Causes, Diagnosis
Causes for psoriatic arthritis:
The exact causes are not clearly known yet
A number of genetic associations have been identified in a genome-wide association study of psoriasis and psoriatic arthritis including HLA-B27
Diagnosis of psoriatic arthritis:
There is no definitive test to diagnose psoriatic arthritis. Symptoms closely resemble other painful conditions like Rheumatoid arthritis. Association with psoriasis will clinch the diagnosis. Thorough case history, physical examination, blood tests and X-rays will help in diagnosing psoriatic arthritis and also to differentiate this condition from other diseases.
Factors contributing to a diagnosis of Psoriatic Arthritis:
- Family history of psoriasis or psoriatic arthritis
- Negative test result for RA Factor (Rheumatoid factor, blood test associated with Rheumatoid arthritis) which rules our Rheumatoid arthritis
- DIP arthritis – Arthritis symptoms in the distal interphalangeal articulations of hand (joints closest to the tips of the fingers)
- Finger and toenail changes – ridging or pitting of fingernails or toenails (onycholysis) associated with psoriasis and psoriatic arthritis
- Radiological images indicating joint change
- Inflammation of Achilles tendon (back of the heel)
- Plantar fasciitis (pain at the bottom of the foot)
- Dactylitis (sausage like swelling of fingers and toes)
Classification
Classification of Psoriatic Arthritis –
Asymmetric arthritis – affects 70% of patients, symptoms are generally mild in nature. It involves less than 3 joints. Same joints on both sides of the body are usually not afflicted, there is asymmetry.

Symmetric arthritis – occurs in 25% cases, affects joints on both sides of the body simultaneously, there is symmetry of presentation. This condition resembles Rheumatoid Arthritis. It is disabling in more than 50% of cases.
Arthritis mutilans – affects less than 5% of patients. It is a severe form of deforming and destructive arthritis. Joint destruction takes place. This condition progresses for months and years and consequentially ends up in joint damage. It is also called as chronic absorptive arthritis.
Spondylitis – characterized by stiffness of the spine or neck. It also affects hands and feet and the presentation is just like symmetric arthritis.
Distal Interphalangeal Predominant Arthritis – This type is found to occur in about 5% of patients and is characterized by inflammation and stiffness of joints nearest to the ends of your fingers and toes. Nail changes are often marked.
Differential diagnosis
Differential Diagnosis of Osteoarthritis:
Osteoarthritis – Osteoarthritis occurs from the breakdown of your protective joint cartilage and underlying bone. OA can affect and damage any joint in the body. Joints of the hands, Joints near the finger ends, base of the thumb, neck, lower back, hips, knees and spine are commonly afflicted by osteoarthritis.
The most common symptoms are joint pain and stiffness. Joint swelling and decreased range of movements are also present in many cases. Other symptoms include tenderness, loss of ability to perform activities, crackling noise (crepitus) when the joint is moved or touched, muscle spasms and contractions in the tendons, fluid in the joint etc. In later stages hard bony enlargements (nodes) are formed.
Gout – Onset of arthritis in gout is usually more acute and over a period of a few hours, but could mimic an exacerbation of acute OA. Gout or pseudogout often co-exists in the same joint. In acute attacks, the affected joint is usually red, hot and tender. Gout commonly involves the foot, especially the first metatarsophalangeal (MTP) joint. It may affect almost any joint.
Rheumatoid Arthritis – RA usually causes a symmetrical small joint polyarthritis in the hands, particularly affecting the Metacarpo-Phalangeal joints. It spares the Distal Interphalangeal joints. Typically RA is associates with morning stiffness which is more prolonged than in OA. There is a feeling of being unwell associated with low mood and fatigue.
Bursitis – Greater trochanteric bursitis in the hip and pes anserine bursitis in the knee present with pain over the lateral aspect of the hip and over the medial aspect of the knee respectively. There is also local tenderness in these areas that is usually absent in simple OA.
Avascular Necrosis (AVN) – This is common in the hip and knee joints. The onset is subacute and there is usually a risk factor such as corticosteroid use. Early in the disease, the joint examination is unremarkable, except for possible localised bony tenderness in the knee.
Internal derangements (ex. meniscal tears) – The onset meniscal tears is usually acute and debilitating, with preceding trauma can be minor. Patients may describe true locking (normal flexion, but an inability to extend the affected knee).
Treatment
Treatments for psoriatic arthritis:
Combating inflammation – Target of treatment will be reducing and controlling the inflammation because the underlying process of psoriatic arthritis is inflammation.
NSAID’s – Non-steroid anti-inflammatory drugs are used to treat milder cases of psoriatic arthritis. NSAID’s include ibuprofen and naproxen. Potent NSAID’s like diclofenac, indomethacin and etodolac are also used when pain is severe. Coxibs (COX-2 inhibitors) example, Celecoxib, Etoricoxib etc are also prescribed.
Disease modifying anti-rheumatic drugs (DMARD’s) and or biological response modifiers – are used to prevent irreversible joint destruction, they are brought into use much earlier in the disease
DMARD’s (Disease Modifying Anti-Rheumatic Drugs) – are used in persistent symptomatic cases without exacerbation. Apart from reducing pain and inflammation, they help limit the amount of joint damage. Example – methotrexate or leflunomide, cyclosporine, azathioprine and sulfasalazine.
Biological Response Modifiers – or biologics target specific parts of immune systems unlike DMARD’s which affect the entire immune system. They are given by injection or intravenous infusion (IV). Example – TNF-a inhibitors, including infliximab, etanercept, golimumab, certolizumab pegol and adalimumab as well as the IL-12/IL-23 inhibitor ustekinumab
Low level laser therapy – has found to relieve pain and stiffness associated with RA, also useful in Psoriatic arthritis
Retinoid etretinate – effective for both arthritis and skin lesions
Photochemotherapy with methoxy psoralen and long wave ultraviolet light (PUVA) are used for severe skin lesions
Joint injections with corticosteroids – when one joint is involved
Orthopaedic surgery with use of joint replacement – to correct joint destruction in severe joint damage associated with psoriatic arthritis
Surgery – effective for pain alleviation correcting joint disfigurement and reinforcing joint usefulness and strength
Epidemiology
70% people of people who develop psoriatic arthritis first show signs of psoriasis on skin, 15% develop both at the same time and 15% develop skin psoriasis following the onset of psoriatic arthritis
It can develop in people who have any level of severity of psoriasis (mild to severe psoriasis)
Psoriatic arthritis tends to appear about 10 years after first signs of psoriasis. For majority of people this will be between ages of 30 and 55 years. The disease also affects the children. Onset of psoriatic arthritis symptoms before skin psoriasis is more common in children than in adults.
More than 80% of patients with psoriatic arthritis will have nail lesions (pitting, separation of nail, ridging, cracking, loss of nail etc)
Men and women are equally affected by this condition
Psoriatic arthritis is more common in Caucasians than Africans or Asians
Click to Consult Dr Raghuram Y.S. MD (Ayu)